


Seizure freedom is the goal. ...but can we know all the risks and obstacles each patient is facing?


SIGNIFICANT CONSEQUENCES
The consequences of breakthrough seizures can be dire―but there are many ways to help mitigate these risks.
HEALTH
Substantial premature mortality from sudden unexpected death in epilepsy (SUDEP), status epilepticus, seizure-related injuries, and suicide3,4
- In neurology, SUDEP is second only to stroke as a cause of total years of potential life lost3,4
- More than 3 convulsive seizures in a year increases risk of SUDEP by a factor of 155
- In one study, most seizure-related injuries were reported for convulsive seizures―42% secondarily generalized, 35% generalized at onset6
- There are many ways to help mitigate the risks of SUDEP―arm your patients with that knowledge
For ideas on how to counsel patients on SUDEP, view the SUDEP Discussion Guide.
RELATIONSHIP
AND SOCIAL
Depression, cognitive decline, and decline in social functioning7-10
- Cognitive decline is strongly correlated with the number of convulsive seizures9
- Children with epilepsy have shown social competency deficiency, memory impairment, depression, and anxiety8,10,11
FINANCIAL
Job loss (with health insurance coverage interruptions), missed work due to comorbidities, and increased treatment costs7,12
Patients with breakthrough seizures had 8.1x higher epilepsy-related costs.12
- Cost of ER visits12
- Loss of ability to work (e.g. driver’s license suspension)7,13

"Patients who do not share a bedroom
and have generalized tonic-clonic seizures
had 67 times the risk of SUDEP."14
Even a brief discussion with patients and their caregivers
about SUDEP may save lives.3

"Some people are on relatively thin ice when it comes to seizure control.
They’re sensitive to small changes in AED blood levels."15
- Jacqueline French, MD, Professor of Neurology at New York University's School of Medicine

"Patients with breakthrough seizures
had 8.1 times higher epilepsy-related
financial costs."14
Help your patients Manage the risks
and Avoid the costs.

KNOWN RISKS
Could understanding patient realities help us guide them toward better outcomes?
Patients have differing needs and challenges, and each breakthrough seizure is a story we don't know. We can't help unless we know what obstacles are getting in the patient's way. Improved quality of life is possible for many people with epilepsy—with help, including education, acknowledgment, and treatment.20
- Living with epilepsy is itself a risk: comorbidities, social stigma, economic difficulties, and psychological and social challenges can be part of the mix.3,18 We should acknowledge these challenges in our treatment plans and take steps to counter them
- Triggers cannot always be avoided. Even when you've prescribed an effective medication, a breakthrough seizure could be triggered by irregular or insufficient sleep, alcohol consumption, and stress22
- A single missed dose can lead to a breakthrough seizure7,23
- Nearly 50% of people with epilepsy surveyed reported having a breakthrough seizure following a missed dose23,*
In one study,
88% of nonadherent epilepsy patients felt uncomfortable telling their doctor about
a missed dose.7
- Patient nonadherence can be a serious obstacle to seizure freedom. For many conditions, 80% adherence is considered acceptable, but in epilepsy the stakes are high and there is very little give with most medications3,12
- Is what we're asking of patients—"near-perfect adherence"—even possible?3 It's important to acknowledge how challenging this is, along with what's at stake
*A 10-item, nationwide postal survey of 661 patients conducted between 2001 and 2002.
Use the Breakthrough Seizure Risk Assessment
Tool as a starting point to discuss your patient's risk
factors for breakthrough seizures.
"I'm facing significant life events
(such as changes to relationships,
moving, a new job)."
HCP RISK ASSESSMENT TOOL
PATIENT RISK ASSESSMENT TOOL


TARGET BREAKTHROUGH SEIZURES
Give patients the tools they need to aim for seizure freedom, so we can move beyond the therapeutic inertia
prevalent in so many chronic conditions.24
Consider a multi-pronged approach to improve risk identification:
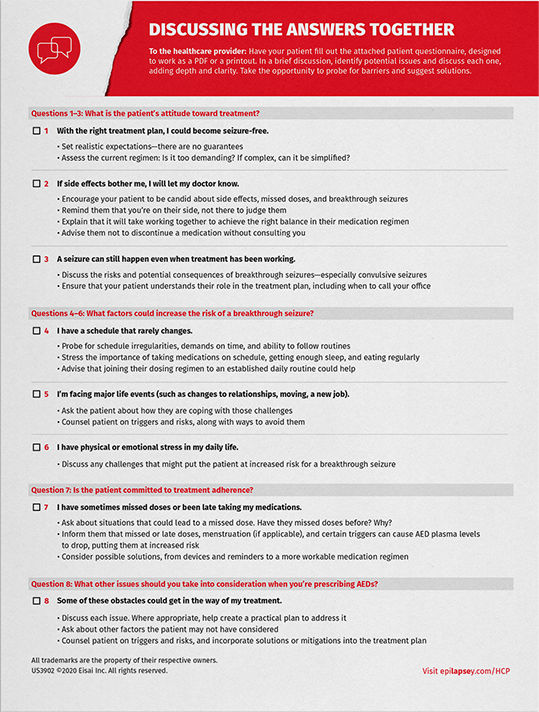
Use the Breakthrough Seizure Risk Assessment Tool to assess your patient, evaluate responses,
and based on patient responses, create a comprehensive, realistic plan of action.7,20
- Establish adherence expectations for your patient
- Prescribe with an eye to patient barriers and challenges—and the likelihood of the patient
keeping medications within a therapeutic range - Set up a timeline for your patient to put plan components in place
- Probe for potential obstacles to seizure freedom, such as:
- A busy and unpredictable schedule
- A stressful job, deadline pressures, or being in school
- Poor diet and inconsistent meal times (sudden changes in metabolism such as a drop in blood sugar or
sodium, and deficiencies in certain nutrients, such as calcium, have all been found to trigger seizures)25,26 - Irregular or insufficient sleep
- Drinking alcohol or taking recreational drugs
- Other physical or mental health issues
- Encourage your patient to report seizures, and discuss any breakthrough seizures they may be having
- Move beyond guilt and shame—understand how challenging "near-perfect" adherence can be
- Work with the patient to create a plan, including:
- A Seizure Plan for caregivers, so they know how to respond and what to do. The Epilepsy Foundation is a useful resource
- Regular check-ins, especially when a new medication is prescribed, or a change is made to the treatment plan
- Adjust the treatment regimen to fit the patient's life. Consider medications:
- With fewer daily doses or once-daily dosing20
- With alternative formulations (i.e. chewable tablet, oral suspension, sprinkle capsules)20
-
Engineered for sustained release or with a long half-life, to help achieve and sustain stable,
steady-state plasma levels that stay within the therapeutic range20,27
-
Suggest that the patient develop reminder strategies to help them increase adherence
and decrease seizure frequency, such as:7,20
- Using a pillbox
- Getting medication reminders via app or email
- Displaying their medication schedules and checking off each dose
Use the Breakthrough Seizure Risk Assessment
Tool as a starting point to discuss your patient's risk
factors for breakthrough seizures.
"What is the patient's attitude
toward treatment?"
HCP RISK ASSESSMENT TOOL
PATIENT RISK ASSESSMENT TOOL


"Everyone with epilepsy and everyone who treats people with epilepsy need to know that controlling seizures will save lives."4
BREAKTHROUGH SEIZURE RISK
ASSESSMENT TOOL
Use this tool with your patients as a quick way to learn
which risk factors for breakthrough seizures are most
prevalent in their lives.
PATIENT RISK ASSESSMENT TOOL


SUDEP DISCUSSION GUIDE
Even a brief discussion with patients and their
caregivers about SUDEP may save lives.3
SUDEP=sudden unexpected death in epilepsy

MANAGE THE RISK,
AVOID THE COST
What are the costs of not managing the risk of
breakthrough seizures? Have these talking points
at hand to share with patients.
Talk with your patients about breakthrough seizures—
especially convulsive seizures.
Some anticonvulsants have a narrow therapeutic range.29 Discuss a treatment
option that may help mitigate some of the risk.